International Society of Urological Pathology
Discussion of case
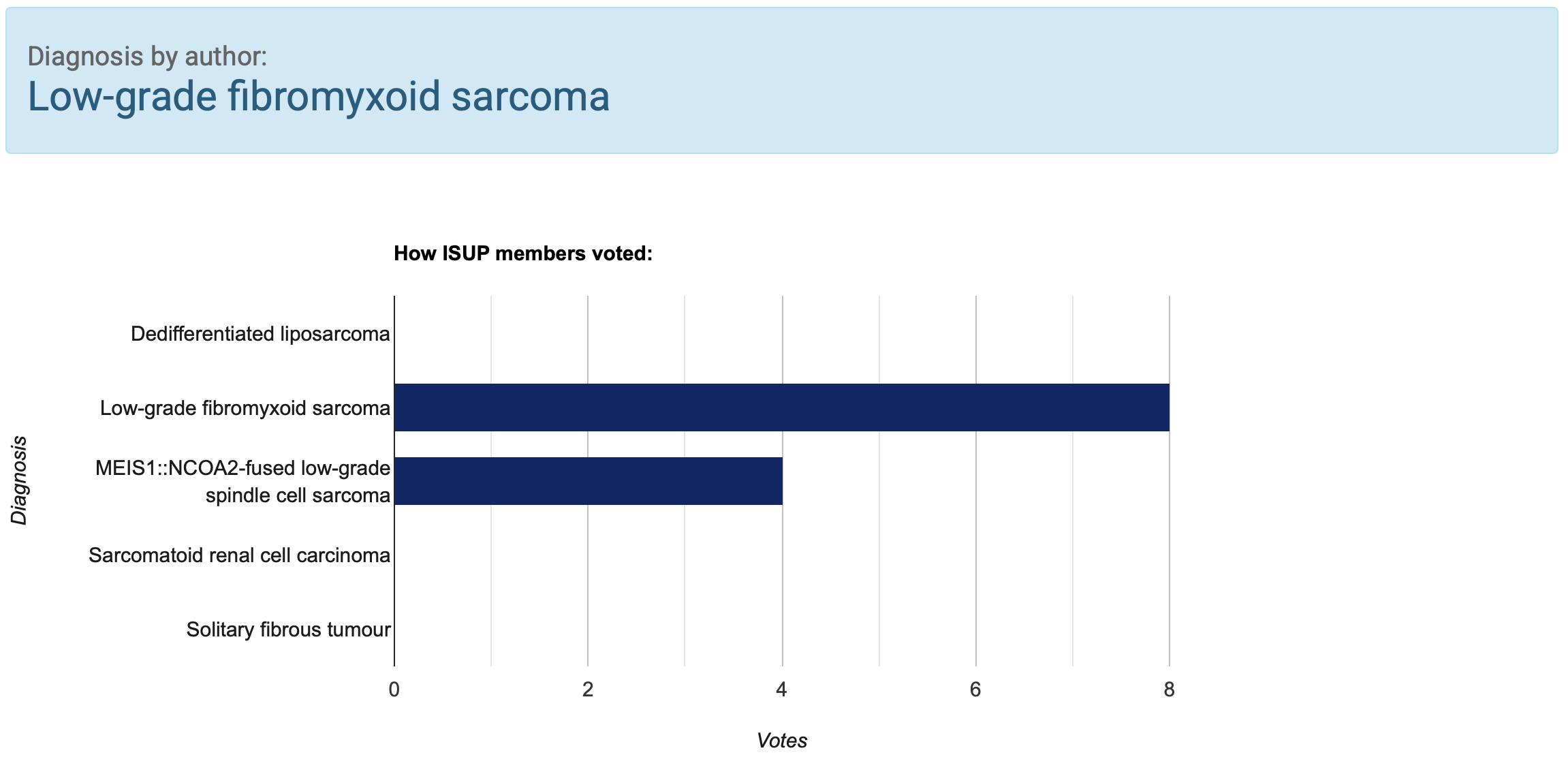
Key differential diagnosis
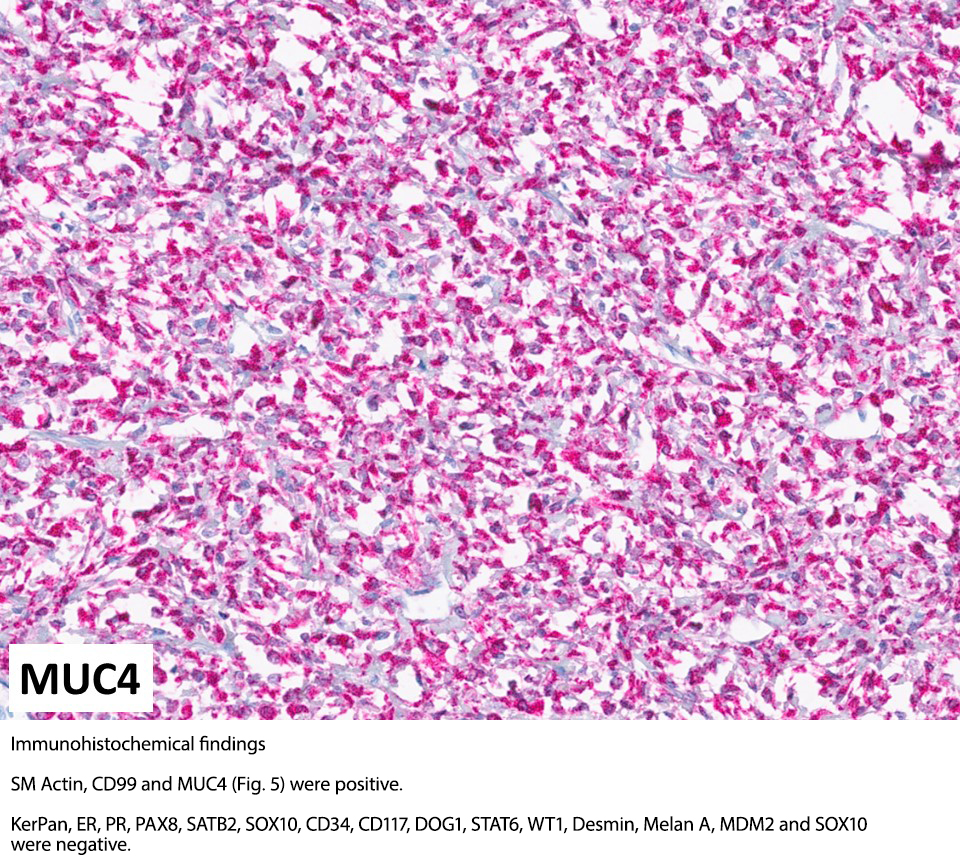
The pitfall of diagnosing LGFMS/SEF is its bland morphology and the absence of immunohistochemical stainings usually performed when encountering low-grade spindle cell lesions in the abdomen and retroperitoneum (CD34, CD117, DOG1, MDM2). MUC4 is a sensitive and specific marker for LGFMS/SEF, and the diagnosis can be confirmed by demonstrating a EWSR1::CREB3L-gen fusion. It is important to be aware LGFMS/SEF can rarely occur as a primary kidney tumour.
Dedifferentiated liposarcoma
Well-differentiated/ dedifferentiated liposarcoma (ddLPS)should always be considered in the differential diagnosis of retroperitoneal and abdominal spindle cell tumours. Mostly it originates within the retroperitoneal fat tissue, but rare primary renal cases have been reported. CDK4 and MDM2 immunohistochemistry and/or FISH are positive and demonstrate MDM2-gene amplification.
MEIS1::NCOA2-fused low-grade spindle cell sarcoma
MEIS1::NCOA2-fused low-grade spindle cell sarcoma is a very rare tumour occurring predominantly in the genito-urinary tract, and particularly within the kidney [4]. The tumour is composed of monomorphic spindle cells and is usually more cellular than LGFMS/SEF with whirling and mitotic activity; however; poorly cellular areas with myxoid stroma can occur. Its immunohistsochemical profile is non-specific, so that molecular fusion analysis is very helpful.
Sarcomatoid renal cell carcinoma
In the majority of cases, sarcomatoid renal cell carcinoma (sarcoRCC) has intermediate to high-grade spindle cells, but in 10% of cases the sarcomatoid spindle cell component is low-grade [5]. The abundance of the spindle cell component can range from 1% to 99% of the tumour. As in all renal cell neoplasms which are difficult to classify, thorough sampling is important. SarcoRCC is expressing PAX8 in about 60% of tumours. With respect to the differential diagnosis of sarcoRCC and ddLPS, be aware that MDM2 is expressed in 60% of sarcoRCC and that MDM2 is amplified in 10% of cases [6].
Solitary fibrous tumour
Solitary fibrous tumour (SFT) can morphologically mimic LGFMS/SEF, being a bland spindle cell lesion with prominent collagenous matrix. Rarely, SFT presents as an intrarenal tumour [7]. Immunohistochemistry (CD34, STAT6, MUC4) and molecular analysis are important for the differential with LGFMS/SEF. With respect to the differential diagnosis of SFT and sarcoRCC, be aware that PAX8 is reported to be expressed in about 30% of SFT and can be expressed diffusely [8].
References
Summary of clinical history
38-year-old female underwent right nephrectomy for a tumour mass
Gross findings
The nephrectomy had a 13-cm large white well-circumscribed mass in the cortex and medulla of the upper pole.
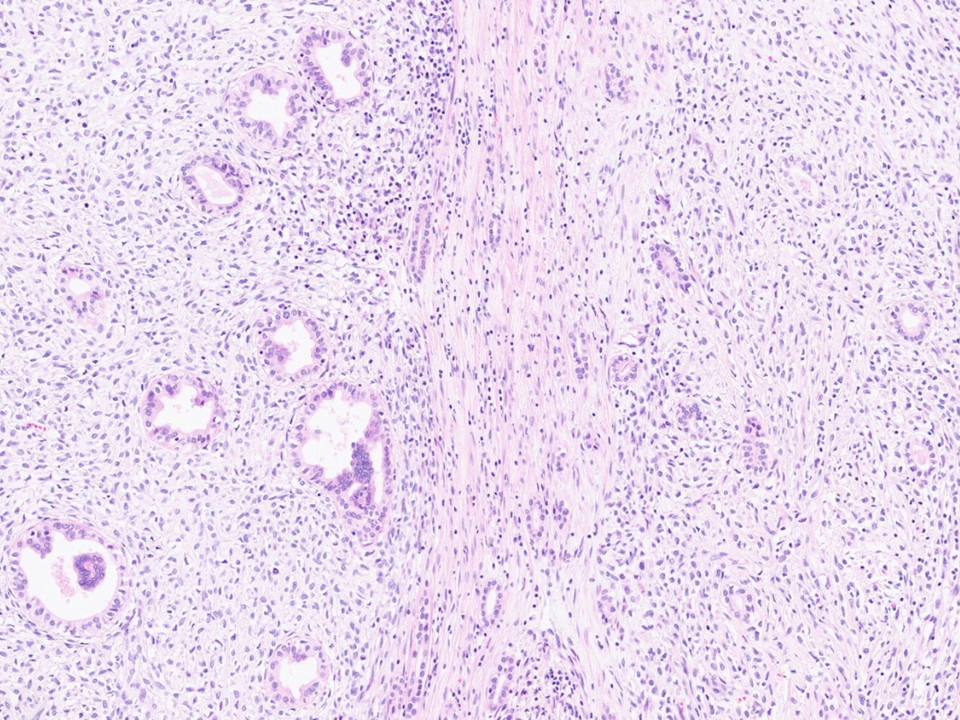
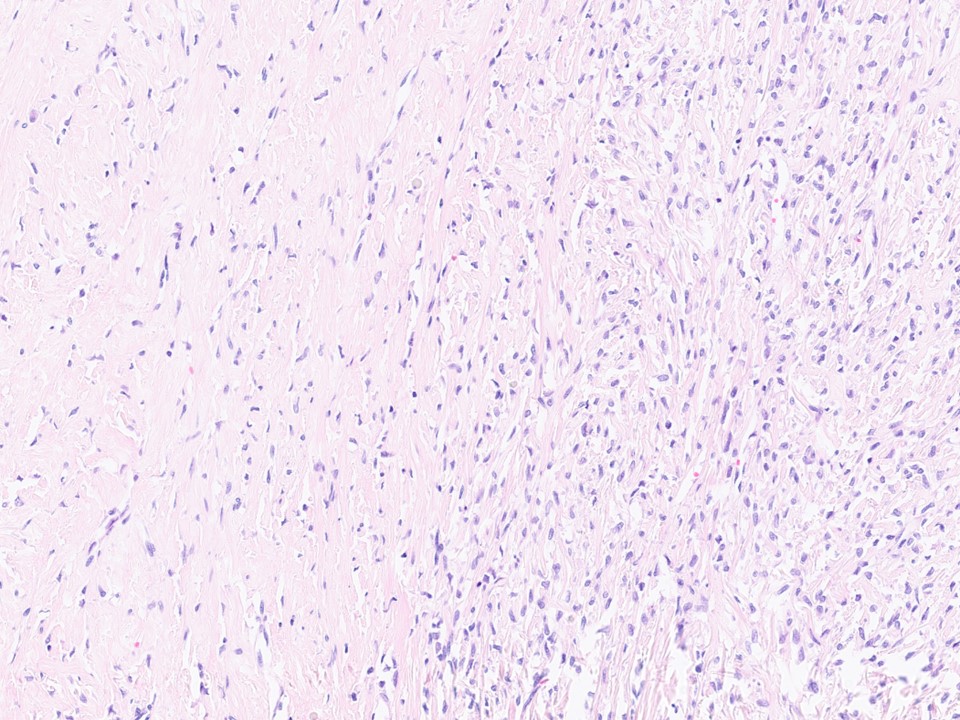
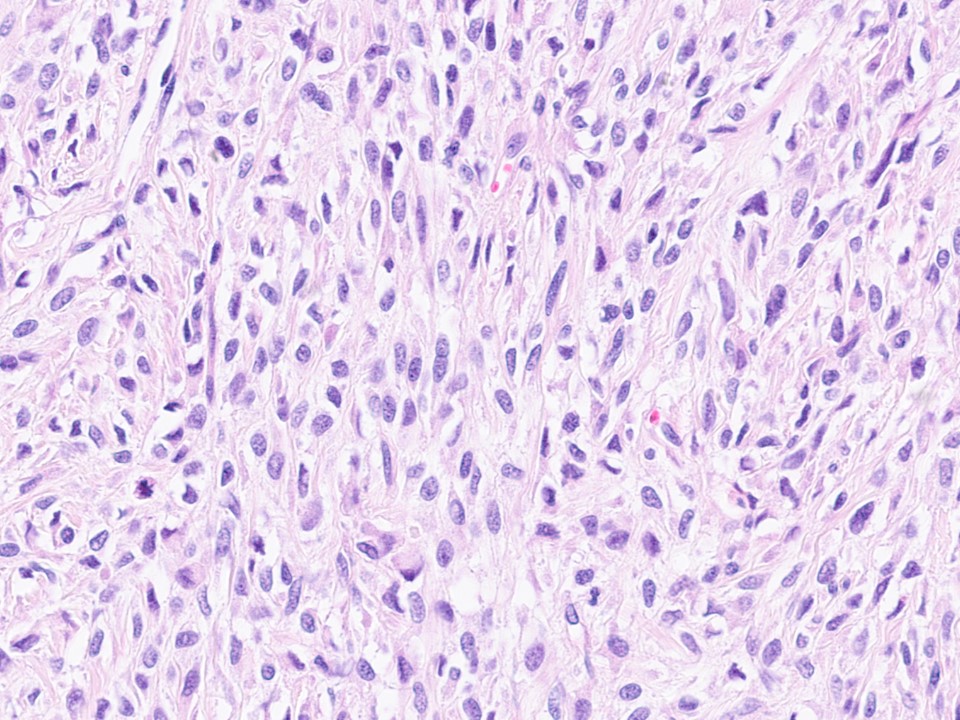
Microscopic findings
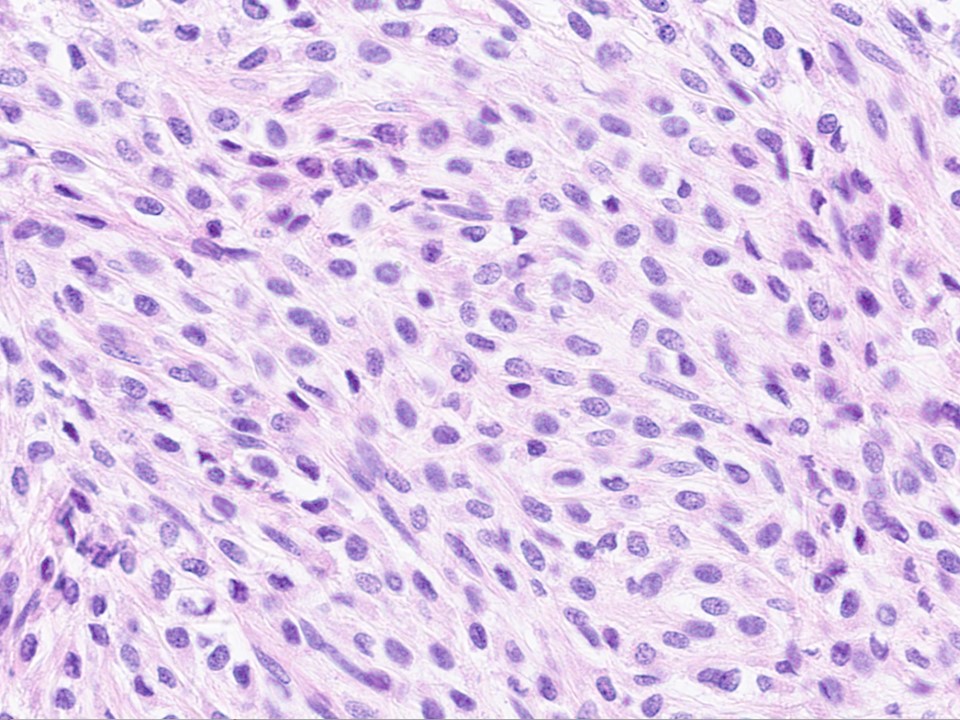
The tumour was unencapsulated and partially extended in between pre-existent renal tubules (Fig. 1). The tumour consisted of vaguely arranged moderately cellular fascicles of spindle cells with eosinophilic cytoplasm, oval nucleus and inconspicuous nucleolus, within an abundant collagenous matrix (Fig. 2). In addition, more cellular areas were present with less elongated to epithelioid cells within a sparse eosinophilic matrix (Fig. 3, 4). There was slight to moderate cellular pleomorphism with sporadic mitotic figures and no necrosis.
CLICK IMAGE TO ENLARGE
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}